 Clinical characteristics, treatment strategies, and long-term outcomes of popliteal artery aneurysms: a single-center retrospective study of 26 patients
Clinical characteristics, treatment strategies, and long-term outcomes of popliteal artery aneurysms: a single-center retrospective study of 26 patients Association between CHA2DS2-VASc score and aortic calcification in patients with atrial fibrillation and its sex-specific predictive value
Association between CHA2DS2-VASc score and aortic calcification in patients with atrial fibrillation and its sex-specific predictive value Extra-anatomic venous bypass using prosthetic grafts for hemodialysis-related symptomatic central venous stenosis: a single-center retrospective study
Extra-anatomic venous bypass using prosthetic grafts for hemodialysis-related symptomatic central venous stenosis: a single-center retrospective study Establishment and preliminary validation of a porcine femoral artery chronic total occlusion-like lesion model induced by combined CaCl2 and FeCl3 treatment
Establishment and preliminary validation of a porcine femoral artery chronic total occlusion-like lesion model induced by combined CaCl2 and FeCl3 treatment Clinical value of a machine learning model integrating ultrasound radiomics and clinical features for predicting pathological complete response to neoadjuvant therapy in HER2-positive breast cancer
Clinical value of a machine learning model integrating ultrasound radiomics and clinical features for predicting pathological complete response to neoadjuvant therapy in HER2-positive breast cancer Development of a prediction model for high Ki-67 expression in invasive breast cancer based on dual-energy CT quantitative parameters
Development of a prediction model for high Ki-67 expression in invasive breast cancer based on dual-energy CT quantitative parameters Clinical value of ultrasound-guided guidewire localization in reoperation for recurrent metastatic lymph nodes after thyroid cancer surgery
Clinical value of ultrasound-guided guidewire localization in reoperation for recurrent metastatic lymph nodes after thyroid cancer surgery Anti-tumor effects and potential mechanisms of oyster glycogen in papillary thyroid carcinoma: a network pharmacology and in vitro experimental study
Anti-tumor effects and potential mechanisms of oyster glycogen in papillary thyroid carcinoma: a network pharmacology and in vitro experimental study Comparison and interpretation of Chinese and international expert consensuses on intersphincteric resection from an anatomical perspective
Comparison and interpretation of Chinese and international expert consensuses on intersphincteric resection from an anatomical perspective Complications and surgical optimization of terminal ileostomy: focus on the one-stitch technique
Complications and surgical optimization of terminal ileostomy: focus on the one-stitch technique Short-term outcomes of circular-stapled esophagojejunostomy after totally laparoscopic versus laparoscopy-assisted total gastrectomy: a propensity score-matched study (with video)
Short-term outcomes of circular-stapled esophagojejunostomy after totally laparoscopic versus laparoscopy-assisted total gastrectomy: a propensity score-matched study (with video) Efficacy and safety of endoluminal vacuum-assisted closure for esophagojejunal anastomotic leakage: a retrospective analysis of 21 cases (with video)
Efficacy and safety of endoluminal vacuum-assisted closure for esophagojejunal anastomotic leakage: a retrospective analysis of 21 cases (with video) Guidelines for the diagnosis and treatment of primary liver cancer (2026 edition)
Guidelines for the diagnosis and treatment of primary liver cancer (2026 edition)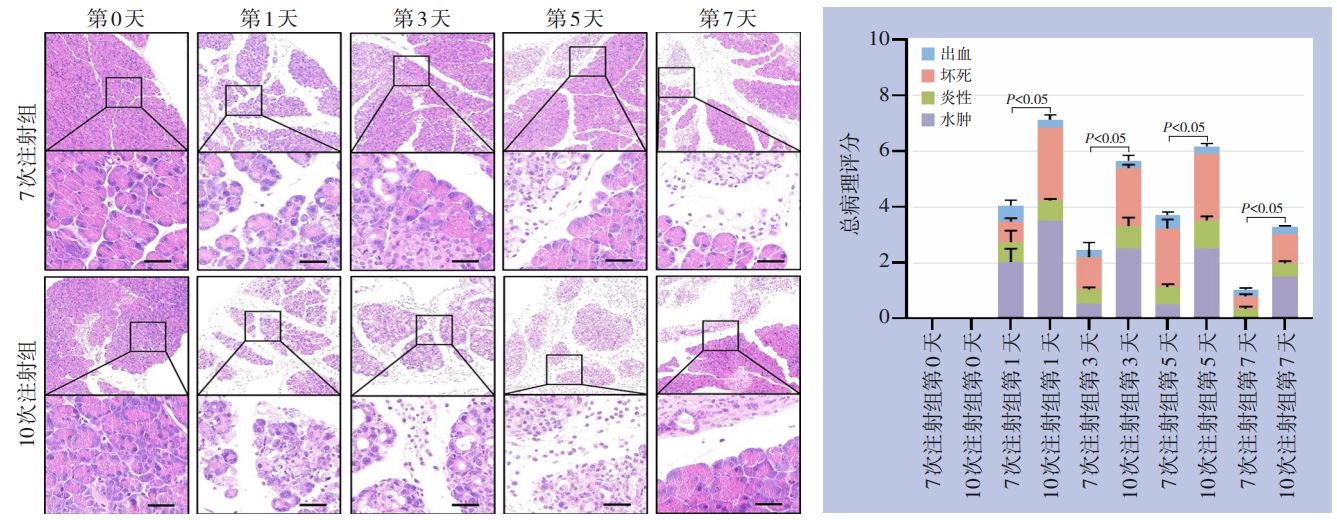 Injury severity-dependent differences in pancreatic regeneration and repair in cerulein-induced acute pancreatitis
Injury severity-dependent differences in pancreatic regeneration and repair in cerulein-induced acute pancreatitis
- Current Issue
- Published Ahead-of-Print
- Virtual Issues
- Previous Issues
-
2026,35(6):1053-1074, DOI: 10.7659/j.issn.1005-6947.260098
Abstract:
Compression therapy is a physical treatment modality that applies continuous or intermittent pressure to specific body regions using compression devices to improve venous and lymphatic return, reduce edema, alleviate symptoms, and promote wound healing. It plays an essential role in the management of venous and lymphatic disorders. However, challenges remain in China, including insufficient high-quality evidence, lack of unified product standards, and non-standardized clinical practice, and evidence-based clinical practice guidelines are still lacking. To address these issues, the Pressure Group of the Peripheral Vascular Disease Professional Committee of the Chinese Society of Microcirculation organized experts from 17 major tertiary hospitals nationwide. Following the Guiding Principles for Developing/Revising Clinical Practice Guidelines in China (2022 Edition) and the RIGHT statement for reporting practice guidelines, the panel developed 32 clinical questions across eight key topic areas. Evidence quality and recommendation strength were assessed using the GRADE approach, and expert consensus was achieved through the Delphi method, resulting in 53 recommendations. This guideline aims to standardize compression therapy for venous and lymphatic diseases in China, improve the scientific rigor and consistency of clinical practice, and promote further research and evidence-based application in this field.
-
2026,35(6):1075-1091, DOI: 10.7659/j.issn.1005-6947.260194
Abstract:
Venous thromboembolism (VTE) is a major preventable cause of morbidity and mortality among hospitalized patients. Although several national guidelines have established general principles for the prevention and management of VTE, practical recommendations for many clinical scenarios remain insufficient, particularly regarding anticoagulation strategies for special thrombotic conditions, timing of ambulation, indications for inferior vena cava filter (IVCF) placement, and interventional therapies. To address these issues and meet regional clinical needs, the Hunan VTE Prevention and Control Alliance and the Special Committee of Thrombosis and Hemostatic Drugs of the Hunan Pharmacological Society convened a multidisciplinary expert panel to develop this consensus. The consensus was formulated in accordance with guideline-development standards using the GRADE approach and a modified Delphi process. A total of 12 key clinical questions were identified, and 30 recommendations were developed, covering VTE prevention, risk assessment, D-dimer application, pharmacological and mechanical prophylaxis, anticoagulation management for special thrombotic conditions, ambulation strategies, IVCF use, and interventional treatment. This consensus aims to provide evidence-based and practice-oriented recommendations for healthcare professionals across Hunan Province, promote standardized VTE management, and facilitate the establishment of a homogeneous regional VTE prevention and treatment system.
- 1
-
2026,35(6):1092-1110, DOI: 10.7659/j.issn.1005-6947.260263
Abstract:
With the rapid aging of the Chinese population, the number of elderly patients undergoing day surgery has continued to increase. Elderly patients are frequently characterized by multimorbidity, polypharmacy, and diminished physiological reserve, placing them at substantially higher perioperative risk than the general adult population. However, there remains a lack of dedicated recommendations for the perioperative management of day surgery in elderly patients, both in China and internationally. To standardize perioperative management for this population, the National Clinical Research Center for Geriatric Disorders (Xiangya Hospital of Central South University), in collaboration with the International Joint Research Center of Minimally Invasive Endoscopic Technology, Equipment and Standards, convened a multidisciplinary panel of experts to develop the Expert consensus on day surgery management for elderly patients (2026 edition) based on a systematic review of the available evidence and extensive clinical experience. This consensus addresses the entire perioperative pathway of day surgery in elderly patients and presents 16 recommendations covering key aspects, including preoperative eligibility assessment, preoperative optimization, intraoperative anesthesia management, perioperative temperature management, enhanced postoperative recovery, discharge management, and post-discharge follow-up. The consensus aims to provide scientific, standardized, and practical guidance for clinical practice across healthcare institutions, improve the safety and quality of day surgery for elderly patients, and promote the standardized implementation of day surgery in the elderly population.
-
HE Saiqi, PAN Haizhou, LIU Chong, WANG Hengzhen, HU Haidi
2026,35(6):1111-1119, DOI: 10.7659/j.issn.1005-6947.260150
Abstract:
Cervical vascular injuries (CVIs), including blunt cerebrovascular injury (BCVI) and penetrating cervical vascular injury, are among the most challenging emergencies encountered in trauma surgery because of their distinct diagnostic and therapeutic characteristics. In 2026, the American Association for the Surgery of Trauma and the World Society of Emergency Surgery jointly published the first evidence-based guidelines for the diagnosis and management of CVIs. The guidelines comprehensively update current recommendations on screening, imaging evaluation, antithrombotic therapy, endovascular intervention, and management of penetrating cervical vascular injuries. Major advances include shifting the management of BCVI from symptom-driven diagnosis to proactive screening of high-risk patients, establishing antithrombotic therapy as the cornerstone of treatment while restricting endovascular intervention to selected indications, and replacing the traditional anatomical zone-based approach for penetrating injuries with a hemodynamic- and clinical sign-based "no-zone" strategy. This review systematically interprets the key recommendations and supporting evidence of the guidelines and discusses their applicability in the Chinese clinical setting in light of the high burden of cerebrovascular disease in China. It is expected to provide a useful reference for the standardized diagnosis and management of cervical vascular injuries in clinical practice.
- 1
- 2
-
2026,35(6):1120-1127, DOI: 10.7659/j.issn.1005-6947.260221
Abstract:
With advances in endovascular techniques and devices, thoracic endovascular aortic repair and endovascular aneurysm repair have evolved from relatively standardized procedures to complex multibranched reconstruction strategies, including fenestrated, branched, parallel-graft, and physician-modified endograft techniques. Compared with standard endovascular repair, complex endovascular aortic repair usually involves longer aortic coverage, incorporation of multiple target vessels, more frequent guidewire and catheter manipulations, and greater device dependence. Accordingly, the spectrum of perioperative severe complications has changed substantially. In addition to conventional complications such as endoleak and stent-graft migration, target-vessel loss or injury, access-related vascular injury, cardiac and cerebrovascular events, spinal cord ischemia, aortic rupture or new-onset dissection, and device-related failure may markedly compromise procedural safety and long-term outcomes. The success of complex endovascular aortic repair depends not only on appropriate procedural planning and technical execution, but also on the ability to identify, prevent, and promptly manage complications. This review focuses on severe perioperative complications associated with complex endovascular aortic repair. Based on recent guidelines, published evidence, and clinical experience, it summarizes the mechanisms, risk factors, preventive strategies, and management principles of major complications. A whole-process management strategy centered on meticulous preoperative assessment, standardized intraoperative manipulation, dynamic perioperative monitoring, and multidisciplinary collaboration is emphasized to improve the safety and clinical effectiveness of complex endovascular aortic repair.
- 1
- 2
- 3
-
TIAN Hongyan, ZHANG Yiman, MA Qiang, MENG Yan
2026,35(6):1128-1138, DOI: 10.7659/j.issn.1005-6947.260249
Abstract:
Acute pulmonary embolism (APE) is one of the most severe forms of venous thromboembolism and is characterized by abrupt onset, rapid progression, and high mortality. Reperfusion therapy is a key strategy for improving outcomes in patients with high-risk and selected intermediate-high-risk APE. Although systemic thrombolysis can rapidly restore pulmonary perfusion and reduce right ventricular overload, its clinical use is limited by a substantial risk of bleeding and multiple contraindications. In recent years, with the refinement of risk stratification strategies, the establishment of pulmonary embolism response teams, advances in catheter-based interventions, and the rapid development of dedicated devices, catheter-directed therapy has attracted increasing attention and has gradually evolved from a rescue treatment into an important risk-stratified therapeutic option. Current interventional approaches for APE mainly include catheter-directed thrombolysis, pigtail catheter thrombus fragmentation, manual aspiration thrombectomy, and percutaneous mechanical thrombectomy, among which mechanical thrombectomy has developed most rapidly. Several imported systems, including Indigo, FlowTriever, and AlphaVac, as well as domestically developed devices such as Tendvia, have been introduced into clinical practice. Available evidence suggests that these techniques can rapidly reduce thrombus burden, improve right ventricular function, and stabilize hemodynamics while minimizing or avoiding the use of thrombolytic agents. This article reviews current guideline recommendations, technological advances, device development and clinical applications of interventional therapy for APE, discusses its use in special clinical scenarios and existing challenges, and highlights future directions for research and clinical practice.
- 1
-
ZHANG Xiong, LI Ming, YANG Chenzi, HE Hao, SHU Chang
2026,35(6):1139-1147, DOI: 10.7659/j.issn.1005-6947.250484
Abstract:
Background and Aims Popliteal artery aneurysm (PAA) is the most common peripheral arterial aneurysm and may result in acute limb ischemia due to thrombosis or distal embolization. Evidence regarding the clinical characteristics and long-term outcomes of PAA in Chinese populations remains limited. This study aimed to evaluate the clinical features, treatment strategies, and long-term outcomes of surgically treated PAA patients at a single center.Methods Patients with PAA who underwent surgical treatment at the Department of Vascular Surgery, the Second Xiangya Hospital of Central South University between January 2018 and December 2024 were retrospectively reviewed. Baseline characteristics, operative details, perioperative outcomes, and follow-up data were collected. Limb salvage, primary patency, and secondary patency were estimated using Kaplan-Meier analysis. Primary patency was further compared between great saphenous vein grafts and prosthetic grafts.Results A total of 26 patients involving 30 limbs were included. The cohort comprised 18 men (69.2%) with a mean age of (59.2±14.2) years. Bilateral lesions were identified in 6 patients (23.1%), and concomitant aortic or iliac aneurysms were present in 6 patients (23.1%). Twenty-four limbs (80.0%) had true aneurysms, and six (20.0%) had pseudoaneurysms. Open surgical repair was performed in 28 limbs (93.3%), whereas endovascular repair was performed in 2 limbs (6.7%). Open procedures included prosthetic graft reconstruction in 16 limbs (53.3%), great saphenous vein grafting in 6 (20.0%), end-to-end anastomosis in 5 (16.7%), and arterial repair in 1 (3.3%). The 30-day complication rate was 10.0%, and no perioperative deaths occurred. The median follow-up duration was 60.0 (19.5-81.3) months. Limb salvage rates were 100.0% at 6 months, 1 year, and 3 years, and 93.8% at 5 years. Primary patency rates were 92.8%, 92.8%, 92.8%, and 86.7%, while secondary patency rates were 96.2%, 96.2%, 96.2%, and 89.3%, respectively. The 6-year primary patency rate was 100.0% in the great saphenous vein group and 53.1% in the prosthetic graft group, without a statistically significant difference (P=0.208).Conclusion Patients with PAA demonstrate a substantial prevalence of bilateral disease and concomitant aortic aneurysmal disease, highlighting the importance of comprehensive vascular screening. Open repair remains safe and effective, and autologous great saphenous vein grafts should be preferred whenever feasible. Endovascular repair may serve as an alternative option in selected patients, although further studies are required to clarify its long-term durability.
- 1
- 2
-
LIU Yuanyuan, ZHANG Yuanyuan, WANG Yawen, LIU Yuhua
2026,35(6):1148-1160, DOI: 10.7659/j.issn.1005-6947.260224
Abstract:
Background and Aims Abdominal aortic aneurysm (AAA) is a common vascular disorder associated with substantial morbidity and mortality. Although physical activity and exercise training have well-established benefits in cardiovascular diseases, their associations with AAA risk and clinical outcomes remain incompletely understood. This study aimed to investigate the dose-response relationship between physical activity and AAA risk and to evaluate the effects of exercise training on exercise capacity, aneurysm progression, and perioperative outcomes in patients with AAA.Methods PubMed, Embase, and the Cochrane Library were searched for prospective cohort studies and randomized controlled trials (RCTs) investigating physical activity or exercise interventions in AAA up to December 13, 2025. Robust error Meta-regression (REMR) was used to assess the dose-response relationship between physical activity and AAA risk. Random-effects meta-analysis was performed for RCTs, and pooled effects were expressed as standardized mean differences (SMD) with 95% confidence intervals (CI).Results Sixteen studies were included. Four prospective cohort studies involving 94 109 participants were eligible for dose-response analysis. Physical activity was linearly associated with a lower risk of AAA occurrence or screening detection (P for non-linearity=0.582), with a 14% reduction in risk for every 20 metabolic equivalent of task (MET)-hour/week increase in physical activity. Six RCTs demonstrated that exercise training did not increase aneurysm diameter (SMD=-0.03, 95% CI=-0.29-0.24, P=0.85), but significantly improved MET levels at both 3 months (SMD=0.49, 95% CI=0.20-0.78, P<0.001) and 12 months (SMD=0.71, 95% CI=0.47-0.96, P<0.001). No significant effects were observed on blood pressure, BMI, or serum MMP-9 levels. In perioperative patients, preoperative exercise-based prehabilitation significantly reduced the length of hospital stay (SMD=-0.75, 95% CI=-1.08- -0.42, P<0.001).Conclusion Higher levels of habitual physical activity are associated with a lower risk of AAA. In patients with small AAA, long-term exercise training appears safe and improves exercise capacity without accelerating aneurysm growth. In patients undergoing AAA repair, preoperative exercise-based prehabilitation may facilitate postoperative recovery and shorten the hospital stay.
- 1
- 2
- 3
- 4
- 5
- 6
-
ZHU Xuanmeng, XIE Wei, MA Tianqi
2026,35(6):1161-1172, DOI: 10.7659/j.issn.1005-6947.260032
Abstract:
Background and Aims Abdominal aortic aneurysm (AAA) is a life-threatening vascular disease closely associated with chronic inflammation and insulin resistance (IR). The C-reactive protein-triglyceride-glucose index (CTI), a novel composite biomarker integrating inflammatory and metabolic status, has shown prognostic value in cardiovascular diseases. However, its association with AAA risk remains unclear. This study aimed to investigate the relationship between CTI and incident AAA using data from the UK Biobank.Methods A total of 315 003 participants free of aneurysmal disease at baseline with available CTI data were included from the UK Biobank cohort. Incident AAA was defined as the primary outcome. Kaplan-Meier analysis was used to estimate the cumulative incidence of AAA across CTI levels, while multivariable regression models and restricted cubic spline (RCS) analysis were employed to evaluate the association between CTI and incident AAA risk and to assess the dose-response relationship. Subgroup and sensitivity analyses were conducted to assess the robustness of the findings.Results During a median follow-up of 16.37 years, 1 343 participants developed AAA. Kaplan-Meier curves demonstrated a progressive increase in cumulative AAA incidence across CTI quartiles. In the fully adjusted model, each standard deviation increase in CTI was associated with a 39% higher risk of AAA (HR=1.39, 95% CI=1.30-1.48). Compared with the lowest CTI quartile, participants in the highest quartile had a significantly elevated risk of AAA (HR=2.15, 95% CI=1.73-2.66; Ptrend<0.001). RCS analysis revealed a significant nonlinear association between CTI and AAA risk (Pnon-linear=0.008). The association was more pronounced among current or former smokers, participants with HbA1c<48 mmol/mol, and those without hypertension, diabetes, coronary heart disease, or lipid-lowering medication use (all Pinteraction<0.05). Sensitivity analyses yielded consistent results.Conclusion Elevated CTI was independently associated with an increased risk of incident AAA in a dose-dependent manner. CTI may serve as a readily available biomarker for early risk identification and risk stratification of AAA.
- 1
- 2
-
WU Tian, SHI Can, LIAN Huilin, CHEN Songhua, ZHANG Siyi, GUO Ren, LI Xiaomin, LI Dai
2026,35(6):1173-1180, DOI: 10.7659/j.issn.1005-6947.250379
Abstract:
Background and Aims Aortic calcification is an important risk factor for adverse cardiovascular outcomes and aortic diseases. However, effective tools for assessing the risk of aortic calcification in patients with atrial fibrillation (AF) remain limited. The CHA2DS2-VASc score is widely used for stroke risk stratification in AF, but its association with aortic calcification has not been fully elucidated. This study aimed to investigate the relationship between the CHA2DS2-VASc score and aortic calcification and to evaluate its predictive value in patients with AF.Methods A total of 1 538 patients with AF who underwent multi-slice computed tomography (MSCT) at the Third Xiangya Hospital, Central South University between February 2015 and February 2022 were retrospectively included. Patients were classified into aortic calcification and non-calcification groups according to MSCT findings. Receiver operating characteristic (ROC) curve analysis was performed to determine the optimal cut-off values of the CHA2DS2-VASc score for predicting aortic calcification. Multivariable logistic regression analysis was used to evaluate the independent association between the CHA2DS2-VASc score and aortic calcification.Results Aortic calcification was identified in 1 251 patients (81.3%). Compared with the non-calcification group, patients with aortic calcification were older and had higher prevalences of hypertension, diabetes mellitus, coronary artery disease, cerebral infarction, and heart failure (all P<0.05). The CHA2DS2-VASc score was significantly higher in the calcification group [3.0 (2.0-4.0) vs. 1.0 (0-2.0), P<0.001]. The prevalence of aortic calcification increased progressively with increasing CHA2DS2-VASc scores (P for trend <0.001). ROC analysis demonstrated that the optimal cut-off value was 2 points in men (AUC=0.737, 95% CI=0.697-0.776) and 3 points in women (AUC=0.730, 95% CI=0.673-0.787). Multivariable logistic regression showed that each 1-point increase in the CHA2DS2-VASc score was independently associated with a higher risk of aortic calcification (OR=1.912, 95% CI=1.638-2.232, P<0.001). Male patients with a score ≥2 and female patients with a score ≥3 had significantly increased risks of aortic calcification [OR=5.528 (95% CI=3.240-9.434) and 9.295 (95% CI=4.390-19.681), respectively; both P<0.001].Conclusion The CHA2DS2-VASc score is significantly associated with the risk of aortic calcification in patients with AF and demonstrates good predictive performance. Sex-specific thresholds of ≥2 for men and ≥3 for women may facilitate risk stratification and early identification of patients at high risk for aortic calcification.
- 1
- 2
- 3
-
WANG Mo, LU Peng, LI Quanming, SHU Chang, ZHOU Yang, WANG Tun
2026,35(6):1181-1189, DOI: 10.7659/j.issn.1005-6947.260029
Abstract:
Background and Aims Central venous stenosis (CVS) is an important cause of hemodialysis access dysfunction. For patients with complex CVS who have failed conservative or endovascular treatment, or whose lesion anatomy is unsuitable for further endovascular intervention, relief of venous hypertension while preserving the existing dialysis access remains challenging. This study aimed to evaluate the safety, effectiveness, and midterm patency of extra-anatomic venous bypass using prosthetic grafts with the internal jugular vein as the outflow tract for hemodialysis-related symptomatic CVS.Methods The clinical data of 25 patients with hemodialysis-related symptomatic CVS who underwent extra-anatomic venous bypass using prosthetic grafts at the Department of Vascular Surgery, the Second Xiangya Hospital, Central South University, between December 2021 and January 2025 were retrospectively reviewed. All patients underwent computed tomography venography of the upper extremity and central venous system before surgery. The inflow and outflow vessels, as well as the bypass route, were individually selected according to the location and extent of the lesion and the venous outflow condition. Perioperative outcomes, symptom relief, complications, and graft patency were assessed. Primary and secondary patency rates were estimated using the Kaplan-Meier method.Results Technical success was achieved in all 25 patients. The procedures included cephalic vein-to-ipsilateral internal jugular vein bypass in 7 patients, cephalic vein-to-contralateral internal jugular vein bypass in 6 patients, axillary vein-to-contralateral internal jugular vein bypass in 6 patients, axillary vein-to-ipsilateral internal jugular vein bypass in 2 patients, bilateral internal jugular vein bypass in 3 patients, and arteriovenous graft-to-ipsilateral internal jugular vein bypass in 1 patient. Venous hypertension-related symptoms, including limb, facial, or chest wall swelling, improved markedly after surgery. The difference in forearm circumference between the affected and contralateral limbs and venous pressure during hemodialysis were both significantly reduced after surgery (both P<0.05). One patient developed acute left heart failure and 2 developed wound hematoma; all recovered after appropriate treatment. No perioperative death or graft-related infection occurred. The median follow-up duration was 22 months. During follow-up, 5 patients developed bypass graft occlusion. Anastomotic stenosis occurred in 3 patients and was successfully treated with percutaneous transluminal angioplasty combined with open thrombectomy. The 1-year primary and secondary patency rates were both 86%, while the corresponding 2-year rates were 64% and 74%, respectively.Conclusion Extra-anatomic venous bypass using prosthetic grafts with the internal jugular vein as the outflow tract is a safe and effective option for hemodialysis-related symptomatic CVS. This procedure may preserve the existing dialysis access and relieve venous hypertension in patients with failed conservative or endovascular treatment, or with anatomy unsuitable for further endovascular intervention. Individualized selection of the inflow and outflow vessels is essential for achieving favorable outcomes.
- 1
- 2
- 3
-
2026,35(6):1190-1198, DOI: 10.7659/j.issn.1005-6947.260310
Abstract:
Background and Aims The management of chronic venous disease has gradually shifted from extensive anatomical removal toward hemodynamic-oriented precision treatment. Whether all varicose tributaries should be routinely removed during endovenous radiofrequency ablation (RFA) remains controversial. This study aimed to evaluate the efficacy and safety of hemodynamically guided selective tributary phlebectomy combined with RFA for primary lower extremity varicose veins.Methods A retrospective analysis was conducted on 166 patients with primary lower extremity varicose veins who underwent RFA at Beijing Tongren Hospital, Capital Medical University, between December 2024 and November 2025. According to the tributary treatment strategy, 56 patients underwent RFA with conventional extensive stab phlebectomy (conventional group), whereas 110 patients underwent RFA with hemodynamically guided selective tributary phlebectomy (modified group). Baseline characteristics, perioperative outcomes, postoperative complications, duplex ultrasound findings, the Venous Clinical Severity Score (VCSS), and the Chronic Venous Insufficiency Questionnaire-20 (CIVIQ-20) scores were compared.Results No significant differences were observed between the two groups regarding age, sex, disease duration, preoperative VCSS, or CIVIQ-20 scores (all P>0.05). However, the modified group had a higher proportion of CEAP class C3 patients, whereas CEAP class C2 patients predominated in the conventional group (both P<0.05). Compared with the conventional group, the modified group showed a significantly higher use of local anesthesia, shorter operative time, fewer skin incisions, less intraoperative blood loss, and lower pain scores at 1 h after surgery (all P<0.05). No significant differences were found in ablation time or pain scores before discharge (both P>0.05). At 1 and 3 months after surgery, the incidences of residual varicose veins and subcutaneous induration, as well as duplex ultrasound findings, were comparable between the two groups (all P>0.05). Both groups achieved significant improvements in VCSS and CIVIQ-20 scores compared with baseline (all P<0.05). Although VCSS improvement was less pronounced in the modified group (P<0.05), the improvement in CIVIQ-20 scores was similar between groups (P>0.05).Conclusion Hemodynamically guided selective tributary phlebectomy combined with RFA is a safe and effective treatment for primary lower extremity varicose veins. It achieves comparable short-term clinical outcomes to conventional extensive phlebectomy while reducing surgical trauma, operative time, and blood loss, thereby facilitating perioperative recovery.
-
ZHOU Keqian, DU Sha, ZHANG Jinming, MA Qianchao, ZHU Ting, ZHANG Wan
2026,35(6):1199-1205, DOI: 10.7659/j.issn.1005-6947.260005
Abstract:
Background and Aims Chronic total occlusion (CTO) lesions in peripheral artery disease (PAD) are characterized by complex pathological changes including thrombosis, vascular remodeling, and calcification. Existing animal models are often unable to simultaneously reproduce these features. This study explored the feasibility of establishing a porcine femoral artery CTO-like lesion model using combined focal treatment with calcium chloride (CaCl2) and ferric chloride (FeCl3).Methods One healthy adult white pig was used. The right femoral artery underwent intraluminal CaCl2 perfusion, FeCl3-soaked filter paper application, and additional perivascular CaCl2 injection, while the contralateral femoral artery served as a sham-operated control. Digital subtraction angiography (DSA) and computed tomography angiography (CTA) were performed before modeling and at 2 and 3 months after modeling. Histological changes were evaluated by hematoxylin-eosin (HE) staining at 3 months.Results DSA demonstrated persistent occlusion of the modeled femoral arterial segment at both 2 and 3 months, with small continuous collateral vessels observed in the delayed phase at 3 months. CTA showed severe stenosis or occlusion of the modeled segment, accompanied by intraluminal filling defects and focal high-density shadows on the vessel wall. HE staining revealed thrombus formation and organization, intimal thickening and disruption, disordered arrangement of medial smooth muscle cells, and focal suspected calcium salt deposition-like changes.Conclusion This single-case preliminary feasibility study suggests that combined focal treatment with CaCl2 and FeCl3 can induce a CTO-like lesion in the porcine femoral artery, characterized by persistent luminal occlusion and thrombus organization with focal calcium salt deposition-like changes. This method may provide an exploratory approach for constructing large-animal models of lower-limb arterial chronic occlusion, although its reproducibility and stability require further validation.
- 1
- 2
- 3
- 4
- 5
- 6
- 7
- 8
-
LIU Jiaoyan, LIU Qian, DING Dan, LIU Yongrong, YANG Kaiyan, CHEN Hua, QIN Qin
2026,35(6):1206-1218, DOI: 10.7659/j.issn.1005-6947.260231
Abstract:
Background and Aims Psychological phenotypes may influence tumorigenesis through behavioral changes, neuroendocrine dysregulation, and immune modulation. However, their causal relationships with gastric cancer remain unclear. This study aimed to investigate the potential causal associations of anxiety, depression, neuroticism, and mood swings with gastric cancer risk using Mendelian randomization (MR), and to prioritize candidate genes potentially involved in this process.Methods A two-sample MR framework was applied. European gastric cancer genome-wide association study (GWAS) data were used as the primary outcome dataset. Univariable MR analyses were performed for four psychological phenotypes, including mood swings, anxiety, depression, and neuroticism. Positive findings were further evaluated using an East Asian gastric cancer GWAS dataset and subsequently assessed by multivariable MR and Bayesian model averaging MR (MR-BMA). Candidate genes were prioritized using the Polygenic Priority Score (PoPS) method and further evaluated through differential expression and survival analyses using the GEPIA2 platform.Results Univariable MR analysis demonstrated that only mood swings were significantly associated with an increased risk of gastric cancer, with an IVW estimate of OR=1.708 (95% CI=1.075-2.713, P=0.023). External validation in the East Asian dataset showed a consistent effect direction with borderline statistical significance (OR=1.747, 95% CI=0.999-3.056, P=0.050). MVMR analysis indicated that mood swings remained independently associated with gastric cancer risk after adjustment for anxiety, depression, and neuroticism (OR=3.296, 95% CI=1.089-9.982, P=0.035). MR-BMA analysis identified mood swings as the most important exposure (MIP=0.935, adjusted P=0.012). Sensitivity analyses revealed no substantial evidence of heterogeneity, horizontal pleiotropy, or reverse causality. PoPS analysis prioritized 32 candidate genes, among which ADAM12 and KYNU exhibited differential expression in gastric cancer tissues and were significantly associated with overall survival.Conclusion Genetic evidence suggests that mood swings may represent an important psychological phenotype associated with increased gastric cancer risk and retain an independent association among multiple psychological traits. ADAM12 and KYNU may serve as prioritized candidate genes for future mechanistic studies. These findings provide novel genetic insights into the relationship between psychological factors and gastric carcinogenesis, although the underlying biological mechanisms require further validation.
- 1
- 2
- 3
- 4
- 5
-
2026,35(6):1219-1228, DOI: 10.7659/j.issn.1005-6947.260272
Abstract:
Iliac vein compression syndrome (IVCS) is a major cause of chronic venous disease. However, distinguishing patients who truly require endovascular intervention from those with incidental anatomical compression remains a major challenge in clinical practice. This review systematically summarizes the advances in imaging modalities for the diagnosis of IVCS, including color Doppler ultrasonography, computed tomography venography (CTV), venography, and intravascular ultrasound (IVUS), with particular emphasis on their clinical applications and inherent limitations. Based on recent clinical evidence, the indications supporting endovascular intervention are comprehensively reviewed, including the clinical benefits in patients with severe chronic venous disease, the application of IVUS-derived quantitative thresholds in treatment decision-making, the high prevalence of IVCS among patients with recurrent varicose veins, and the pathophysiological significance of iliac vein compression as an anatomical predisposing factor for deep vein thrombosis. In addition, the rationale for conservative management in patients with well-developed collateral venous circulation, the limited long-term efficacy of stenting in patients with severe stenosis, and the complementary value of functional hemodynamic parameters in guiding treatment decisions are also discussed. Current evidence suggests that treatment decisions based solely on the degree of anatomical stenosis have inherent limitations. A comprehensive assessment integrating clinical symptom severity, quantitative IVUS measurements, and functional hemodynamic evaluation may improve the precision of patient selection for endovascular intervention. Nevertheless, high-quality multicenter prospective studies are still warranted to further optimize the indications for endovascular treatment in patients with IVCS.
- 1
-
XU Zhekai, GUI Liang, ZOU Junjie
2026,35(6):1229-1238, DOI: 10.7659/j.issn.1005-6947.250615
Abstract:
Chronic limb-threatening ischemia (CLTI) represents the most advanced stage of peripheral artery disease, and a subset of patients are considered "no-option" because conventional surgical or endovascular revascularization is not feasible. Deep vein arterialization (DVA) has emerged as a promising limb salvage strategy by redirecting arterial blood into the distal venous system to improve tissue perfusion. With the continuous evolution of open, percutaneous, and hybrid DVA techniques, together with dedicated devices such as the LimFlow system, encouraging improvements have been achieved in technical success, limb salvage, and wound healing. This review summarizes the physiological basis, technical evolution, clinical outcomes, device development, perioperative management, and current challenges of DVA. The advantages and limitations of different techniques are also discussed to provide evidence for optimizing clinical application and future research in patients with no-option CLTI.
- 1
-
CHEN Ke, HU Xianyu, LI Wendong, ZHA Binshan, CHEN Zhiyong
2026,35(6):1239-1250, DOI: 10.7659/j.issn.1005-6947.250580
Abstract:
Venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary thromboembolism (PE), is a common and potentially life-threatening vascular disease. Although D-dimer is widely used for VTE screening, its limited specificity restricts its diagnostic accuracy and clinical utility for risk stratification. In recent years, increasing evidence has demonstrated that a variety of emerging biomarkers may contribute to the early diagnosis, risk assessment, therapeutic monitoring, and prognostic evaluation of VTE. This review summarizes the biological characteristics, molecular mechanisms, and clinical applications of representative biomarkers, including D-dimer, microRNAs, tissue factor pathway inhibitor, neutrophil extracellular traps, fibrin monomer, thrombomodulin, microparticles, ischemia-modified albumin, E-/P-selectins, and galectin-3. The current progress in multimarker combination strategies and their potential clinical applications are also discussed. Future studies should focus on standardized detection methods, prospective validation of multimarker panels, and integration with multi-omics technologies to improve early diagnosis, individualized risk stratification, and precision management of VTE.
-
2026,35(6):1251-1260, DOI: 10.7659/j.issn.1005-6947.260276
Abstract:
Carotid body tumor (CBT) is a rare paraganglioma arising from the carotid bifurcation and is generally characterized by benign biological behavior; however, a subset of patients may develop local invasion, recurrence, or distant metastasis. In recent years, advances in molecular biology and imaging techniques have substantially improved our understanding of the pathogenesis, diagnosis, and management of CBT. Current evidence indicates that chronic hypoxia and mutations in succinate dehydrogenase (SDH)-related genes jointly contribute to tumorigenesis, with SDH mutation-induced pseudohypoxia signaling representing a major research focus. Color Doppler ultrasonography, computed tomography angiography (CTA), and magnetic resonance angiography (MRA) remain the principal imaging modalities for diagnosis and preoperative evaluation. Compared with the traditional Shamblin classification, the Peking Union Medical College Hospital classification incorporates longitudinal anatomical extension, providing more accurate surgical risk stratification for complex tumors. In addition, the Grading System for Adrenal Pheochromocytoma and Paraganglioma (GAPP) facilitates assessment of malignant potential. Surgical resection remains the treatment of choice, whereas perioperative carotid management, preoperative embolization, and endovascular interventions continue to be topics of ongoing debate. Precision radiotherapy serves as an effective alternative for patients who are inoperable or at high surgical risk. This review summarizes recent advances in the pathogenesis, clinical manifestations, classification, diagnosis, treatment, and follow-up of CBT, aiming to provide updated evidence for clinical practice and future research.
- 1
-
XIAO Dan, LI Zhi, HE Hengzheng
2026,35(6):1261-1268, DOI: 10.7659/j.issn.1005-6947.260273
Abstract:
Gastroesophageal reflux disease (GERD) is a common chronic digestive disorder whose pathogenesis involves not only reflux-induced mucosal injury caused by gastric acid and bile acids but also persistent activation of inflammatory and oxidative stress responses. Emerging evidence indicates that reflux stimulation disrupts the esophageal epithelial barrier and promotes excessive generation of reactive oxygen species (ROS), leading to the activation of multiple signaling pathways, including TLR4/MyD88, NF-κB, MAPK, Nrf2, and IL-6/JAK/STAT3. These pathways interact to form an inflammation-oxidative stress network that drives disease progression and Barrett's esophagus development. This review summarizes recent advances in inflammation- and oxidative stress-related signaling pathways in GERD and proposes a stage-specific regulatory model consisting of inflammation initiation, signal amplification, oxidative stress imbalance, and chronic remodeling. Key molecular events and their interactions during disease progression are discussed. In addition, current and emerging therapeutic strategies, including proton pump inhibitors, potassium-competitive acid blockers, mucosal protective agents, and pathway-targeted interventions, are reviewed with respect to their mechanisms of action and research status. This stage-specific regulatory framework may provide new insights into the pathogenesis of GERD and offer a theoretical basis for mechanism-based precision therapy and future drug development.
- 1





















































